"There is art to medicine as well as science, and that warmth, sympathy, and understanding
may outweigh the surgeon’s knife or the chemist’s drug."
Hippocratic Oath
WITHOUT DIGNITY THERE IS NO HEALTH
an integrative approach as complement to classical medical treatment.
Practice Dignity is an integrative clinical care practice centred on patient dignity, clinical listening and responsible care in the face of complexity. It is grounded in a broad understanding of health, not as a purely biological or chemical phenomenon, but as the result of multiple social, relational, cultural and institutional determinants that directly shape people’s bodies and lives.
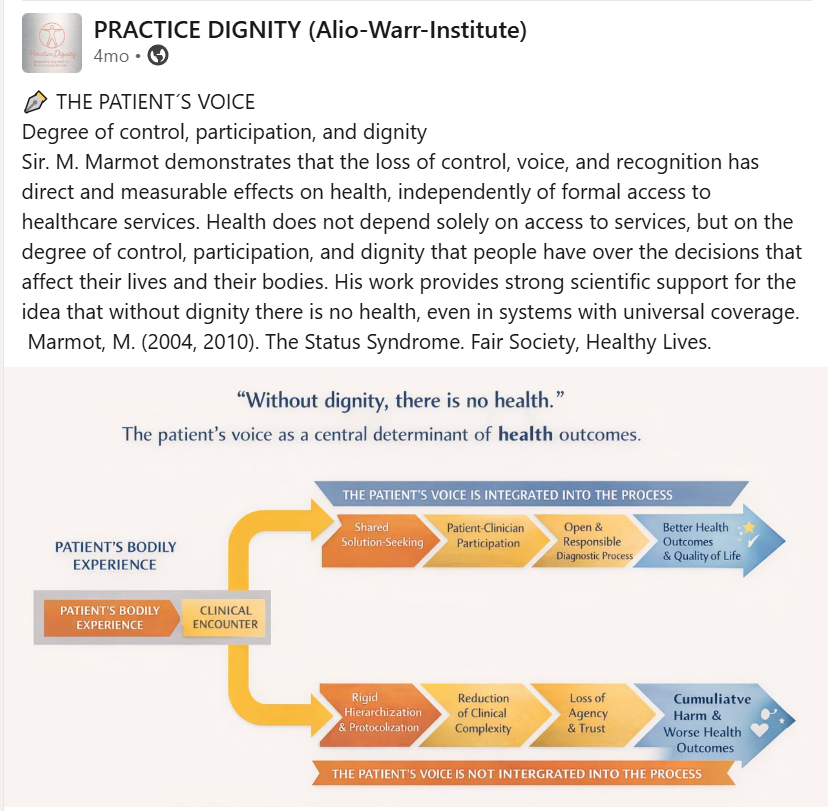
Research in public health and global health has consistently shown that access to health services and technological development, while essential, do not in themselves guarantee safe, equitable or effective care. Health also depends on the degree of control, recognition and real participation that people have in decisions affecting their bodies and life trajectories. When these dimensions are eroded, health deteriorates, even in systems with universal access and high coverage (Marmot, 2004; Marmot, 2010).
Practice Dignity was created to accompany patients living with complex medical trajectories, uncertain diagnoses, persistent symptoms or experiences of invalidation within the health care system. People who feel that their testimony has not been heard, that their bodily experience has been minimised or reductively reinterpreted, or that they have been subjected to early psychiatric labelling and premature diagnostic closure.
From an ethical and clinical perspective, we uphold a central premise. Without dignity there is no health. Patient dignity is not an abstract value or an optional addition to care. It is a central determinant of health outcomes. It involves recognising the patient’s testimony as clinically relevant knowledge, respecting lived bodily experience and ensuring real participation in diagnostic and therapeutic processes.
Michael Marmot has shown consistently that the loss of voice, agency and social recognition is not merely a moral injustice, but a structural determinant of disease, with measurable effects on morbidity, mortality and quality of life (Marmot, 2004; Marmot, 2010). When patients are reduced to passive objects of intervention, even in contexts of material abundance and guaranteed access, health outcomes worsen.
From the field of medical anthropology, Arthur Kleinman has demonstrated that illness experience cannot be reduced to biomedical parameters without producing a significant loss of clinical understanding. When the patient’s narrative is delegitimised, suffering does not disappear. It becomes chronic, intensifies and becomes increasingly difficult to address. Listening to patients is not an optional humanitarian gesture. It is a fundamental clinical condition for understanding what is happening and how to intervene appropriately (Kleinman, 1988; Kleinman, 2006).
Elizabeth Kübler Ross was among the first authors to warn that the failure of medicine lies not only in the inability to cure, but also in the inability to listen. When patient suffering is denied or reinterpreted through rigid frameworks that do not allow for uncertainty or the complexity of human experience, harm not only persists but is amplified. Failing to listen to the patient constitutes an active form of harm, even in the absence of any intention to cause damage (Kübler Ross, 1969; Kübler Ross, 2000).
In line with these perspectives, the World Health Organization emphasises that people centred care and respect for patient dignity are essential components of safe and effective health systems, and that their absence is associated with poorer health outcomes, even in contexts of high coverage (WHO, 2016; WHO, 2021).
Practice Dignity offers a critical, ethical and responsible integrative care model that does not replace conventional medicine, but complements it. Clinical work is grounded in creative therapies and supportive care, with an approach based on needs, proportionality and clinical governance, aimed at preventing avoidable harm and supporting therapeutic processes that respect human complexity.
This practice is addressed both to patients and to professionals, health care teams and institutions. In addition to integrative clinical care, Practice Dignity offers training and consultancy for clinics, institutions and professionals in medicine and the therapeutic fields, with the aim of strengthening models of care centred on the person, dignity and clinical listening. Education in these areas remains a significant gap within Western medicine, despite its direct impact on patient safety, quality of care and health outcomes.
Practice Dignity offers a space to rethink care, to critically examine practices that generate avoidable harm, and to develop forms of attention that integrate scientific evidence, clinical ethics and deep respect for patient experience. A space where the patient’s voice is not an obstacle, but a central source of knowledge and responsible care.
We invite you to explore this project and learn more about its identity, therapeutic approach and work with patients and institutions.

WHAT WE STAND FOR






- All rights reserved Integrative Praxis Erica F. Alio-Warr 2016-2025
- Music & Sound by Amonada Zeon Music
- Logo image Practice Dignity ange 2026